Posterior Retroperitoneoscopic Adrenalectomy
Sanziana Roman MD and Julie Ann Sosa MD MA are among a select few endocrine surgeons in the country who use small incisions to remove adrenal tumors through the back. This avoids painful abdominal incisions and results in a shorter, less invasive operation with faster recovery time.
UCSF endocrine surgeons now offer select patients a new state-of-the-art surgical procedure, posterior retroperitoneoscopic adrenalectomy (PRA), a minimally invasive procedure in which adrenal gland masses are removed through small incisions in the back. In clinical studies, PRA was found to have superior outcomes versus the traditional laparoscopic procedure through the abdomen. Advantages of this approach include:
- Less time in the operating room
- Less blood loss during surgery
- Significantly less scarring
- Reducing the risk of surgical access site herniation
- Less post-operative pain
- Faster recovery and return to normal activities
- A shorter hospital stay
Importantly, PRA was found to be equallly safe when compared with a traditional transabdominal laparoscopic adrenalectomy.
PRA is also especially helpful where:
- Tumors are present in both adrenal glands, observed in 10% of patients
- Patients previously had extensive abdominal surgery
In this case study, Sanziana Roman, MD, an endocrine surgeon who sees patients with disorders of endocrine systems—including thyroid, parathyroid and adrenal gland—discusses a patient’s treatment for a tumor in the retroperitoneum, near the adrenal gland. In consultation with his endocrinologist, surgery was performed minimally invasively through a unique posterior approach that enabled preservation of the kidney and adrenal gland, and allowed for safe removal of the tumor.
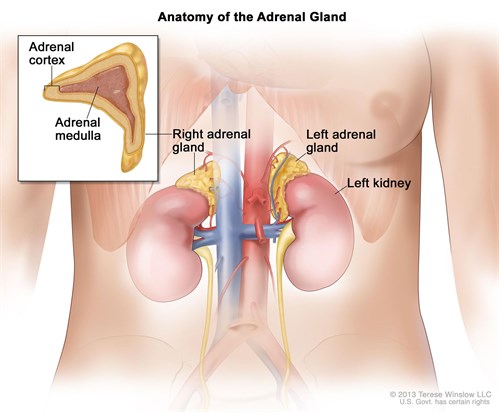
About the Adrenal Glands
Individuals have two adrenal glands each shaped like a triangle, with one siting atop each kidney. Each gland is comprised of two parts, an outer layer called the adrenal cortex, and the center of the gland, called the adrenal medulla. The adrenal cortex makes important hormones including steroids that balance the water and salt in the body and help maintain normal blood pressure. The adrenal medulla makes catecholamines, the hormones epinephrine (adrenalin), norepinephrine, and dopamine.
Although individuals have two adrenal glands, only one normal gland is needed to provide adequate hormonal function. Where both glands must be removed, patients must take steroid supplements of cortisone and hydrocortisone.
Surgical Approach
Minimally Invasive
- Posterior retroperitoneoscopic adrenalectomy (or PRA) requires the patient to lie face down on the operating table. The surgeon will then place a small, lighted camera into the back/flank side through a series of small incisions. This allows the surgeon to view and access the adrenal glands. Small surgical tools are used to remove the entire adrenal gland containing the tumor or, if possible, only a portion of it.
- Transabdominal laparoscopic adrenalectomy If patients are not good candidates for PRA, the surgery is performed laparoscopically through the abdomen using a camera and small instruments.
Open Surgery
If a patient is not an appropriate candidate for minimally invasive adrenalectomy (PRA or transabdominal laparoscopic) then the following alternatives will be recommended:
- Hand-assisted surgery - a hybrid between a fully laparoscopic and open procedure requiring 3-4 incisions that enable the surgeon to insert his/her hand along the small laparoscopic incisions. This method allows for the adrenal gland to be more easily manipulated while still maintaining the operation as a laparoscopic one.
- Open surgery - this approach requires larger incisions, usually in the abdomen, and is indicated for patients:
- With very large adrenal tumors that cannot be accessed and removed laparoscopically
- For tumors that adhere to other organs
Surgical Consultation
Once a diagnosis has been made, the patient has a surgical consultation to determine if surgery is required or whether the condition can be safely monitored without surgery. If an adrenal tumor is identified as an incidental finding (typically found during an unrelated medical procedure), it is critically important that the patient be evaluated to ensure the tumor is not releasing excess adrenal hormones. Imaging studies of the adrenal glands and the tumor are performed and assessed by surgeons who are experts in the evaluation of adrenal masses.
Imaging Tests
CT scans and magnetic resonance imaging (MRI) produce high-resolution three-dimensional (3-D) images of the adrenal glands and are used to assess anatomical structures and reveal abnormalities. Other imaging studies may be performed to determine if the adrenal mass is "functional" (over-secreting hormones) with the goal of minimizing exposure to radiation and any patient discomfort.
Why Choose UCSF for Minimally Invasive Adrenal Surgery
- Unparalleled surgical expertise in the treatment of adrenal masses - UCSF is a high volume tertiary referral center for adrenal surgery. Our world class surgeons frequently see patients other institutions turn away as too risky or complex to operate on. Our surgical teams also see patients with rare tumors and syndromes requiring extensive diagnostic work-up.
- State-of-the-Art Procedures - We offer patients procedures such as PRA where surgery is done through small back incisions. Because the adrenal glands are found above each kidney, the surgeon does not need to move organs out of the way in the abdomen such as the spleen, liver, pancreas and colon. The patient has a faster operation with fewer risks, less blood loss, minimal scarring, less post-operative pain, and a faster recovery.
 Reputation For Excellence - UCSF Medical Center was ranked among the top 10 Adult Diabetes & Endocrinology Hospitals in the U.S. for its 2018 survey. The multidisciplinary endocrine surgery and oncology teams at UCSF provide seemless expert care in diagnosing and treating patients with adrenal masses, whatever their source.
Reputation For Excellence - UCSF Medical Center was ranked among the top 10 Adult Diabetes & Endocrinology Hospitals in the U.S. for its 2018 survey. The multidisciplinary endocrine surgery and oncology teams at UCSF provide seemless expert care in diagnosing and treating patients with adrenal masses, whatever their source.

